- 结合图解自己诊断腰椎间盘突出症和选择治疗方法
- 发布于 2011-09-17 17:34 来源:许国增医生
(原创作品,引用者必须注明来源,否则翻版必究)
1.症状:单纯腰痛伴/或腿痛,腿痛沿坐骨神经分布。疼痛、麻木范围因突出压迫神经根节段不同而异。 广州市番禺区中医院介入科许国增
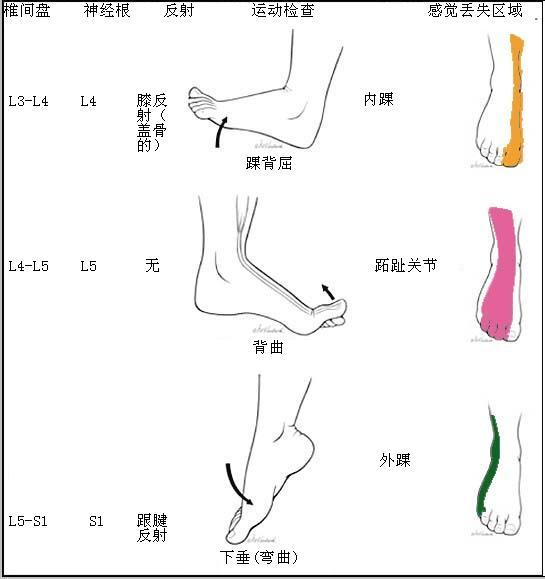
腰5(L5)骶1(S1)神经根受压时,疼痛及感觉减退或麻木区如下图示意
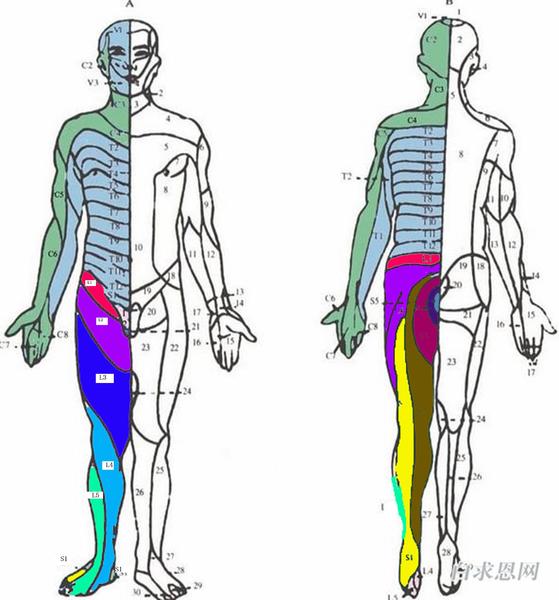
以上图来自网上供参考。需要指出的是,疼痛、麻木区域可较上图标示范围有交叉,故若有上述典型症状,对照CT/MR片可自我诊断,否则最好请专科医生协助诊治,并且可以帮助排除其它疾病,以免延误诊治。
2.体征:需要医生来完成,神经根或马尾神经损伤的阳性体征。
3.CT图像:举例,取自我的研究论文病例。

图. 介入术前,横断位:突出物(双箭)压迫左侧S1神经根,矢状位:显示(脱垂型)非包含型L5/S1椎间盘突出物;冠状位:显示清晰突出物(箭)压迫左侧S1神经根。
对应上彩图S1神经左侧黄色和深绿色感觉丢失区域。
Collagenase chemonucleolysis with left translaminar approach at L5-S1 level in 32-year-old man. (a)Transverse CT image shows left L5-S1 disc herniation material (double arrow), compression of the left S1 nerve root and thickening(long arrow) compared with the contralateral nerve root at the same level , normal right S1 nerve root (arrow), Pfirrmann grading 3. sagittal CT image shows L5-S1 disc herniation material (arrow) with the base of protrusion relative narrower (double arrows) than the diameter of the extruding material itself ; coronal CT image shows L5-S1 disc herniation material (loog arrow),compression of the left S1 nerve root and thickening(double arrows) compared with the contralateral nerve root at the same level , normal right S1 nerve root, Pfirrmann grading 3. (b) After 6 months a reduction lumbar disc herniation material (arrow) and normal S1 nerve root were observed at axial, sagittal and coronal CT imaging , Pfirrmann grading 0.
)
Figure. 介入术后,突出物明显变小,神经根未见受压。
Collagenase chemonucleolysis with left translaminar approach at L5-S1 level in 32-year-old man. (a)Transverse CT image shows left L5-S1 disc herniation material (double arrow), compression of the left S1 nerve root and thickening(long arrow) compared with the contralateral nerve root at the same level , normal right S1 nerve root (arrow), Pfirrmann grading 3. sagittal CT image shows L5-S1 disc herniation material (arrow) with the base of protrusion relative narrower (double arrows) than the diameter of the extruding material itself ; coronal CT image shows L5-S1 disc herniation material (loog arrow),compression of the left S1 nerve root and thickening(double arrows) compared with the contralateral nerve root at the same level , normal right S1 nerve root, Pfirrmann grading 3. (b) After 6 months a reduction lumbar disc herniation material (arrow) and normal S1 nerve root were observed at axial, sagittal and coronal CT imaging , Pfirrmann grading 0.
虽然CT/MR广泛应用,但更好的显示神经根的冠状位等未见应用的报道。它将是今后的应用方向。
症状、体征、CT/MR图像的一致性,诊断明确。进行治疗方法选择。
1,包含型腰椎间盘突出症,首选保守治疗,无效介入治疗。
2,非包含型腰椎间盘突出症,Pfirrmann grading 0-1级,首选保守治疗,无效介入治疗。
3,非包含型腰椎间盘突出症,Pfirrmann grading 2-3级,首选CT导引介入治疗,
无效可手术治疗。
4,不能明确为非包含型腰椎间盘突出症,首选保守治疗。
5,特殊病例需要进一步细分要引入以下四个指标:VAS, A visual analogue scale for pain. ODI, The Oswestry disability index. A-index, the ratio of the area of herniated disc material to the spinal canal. Pfirrmann grading , Pfirrmann’s Grading of lumbar nerve root compromise。要有十分专业医生完成。
非手术治疗:腰椎间盘突出症中约80%的病人可经非手术疗法缓解或治愈。其目的是使椎间盘突出部分和受到刺激的神经根的炎性水肿加速消退,从而减轻或解除对神经根的刺激或压迫(1)。(1)外科学第6版。875-880。
手术治疗:已确诊的腰椎间盘突出症患者,经严格非手术治疗无效,或马尾神经受压者可考虑行髓核摘除术。其有可能发生椎间盘感染、血管或神经根损伤,术后粘连复发等并发症,应严格掌握手术指征(1)。(1)外科学第6版。875-880。
目前治疗腰椎间盘突出症的乱象是,该保守的却进行了介入治疗,放宽了适应症。
而更可怕的是大多数手术治疗的病人可以通过介入治疗来解决,过度手术。
请认真读诊前须知,
如你还有疑问请上传图像,为你诊断。





